
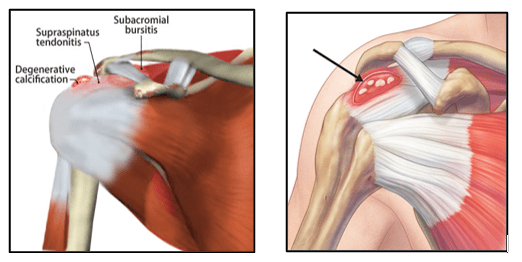
Calcific Tendinitis is a relatively common shoulder condition in which calcium deposit formation occurs within the rotator cuff tendon. The supraspinatus tendon is the most commonly affected tendon of the rotator cuff.
Calcific tendinitis is one of the commonest causes of non-traumatic pain in the shoulder. These calcium deposits occur most commonly in females between 35 and 65 years of age, but males are also affected. Frequently, these calcium deposits do not cause problems, but if they increase in size or become inflamed, then severe pain may arise.
The cause of calcific tendonitis is unclear and is still not completely known. It has been suggested that it may be secondary to tendon degeneration or reduced blood supply within the tendon. It may also possibly be due to genetic influences or a cell mediated response. It is more common in patients having diabetes mellitus and hypothyroidism.
- Pre-calcific stage: There appears to be some initial change in the fibrocartilage cells within the tendon that allows calcium to be deposited within the tendon. This is a painless stage.
- Calcific Stage: This stage has 3 phases
Formative stage: in which chalky calcium deposits form.
This stage tends to be chronic and painless
Resting stage: Calcification has already occurred
There is local inactivity and no inflammation
This stage may last for a varied length of time.
Resorptive stage: The body mounts an inflammatory reaction to the
calcium.
Macrophages from the blood stream react to
the calcium and start to reabsorb the calcium deposit.
The calcium lump becomes soft and toothpaste like due
to the enzymes released by the macrophages.
This stage is usually acutely painful.
- Post Calcific stage: This is usually a painless stage, as the calcium deposits disappear, and it is replaced by a more normal appearing rotator cuff tendon.
The presence of calcium in the rotator cuff tendons is relatively common. Between 2 to 20% of people may have calcium deposits in their rotator cuff tendons without symptoms
The shoulder becomes symptomatic when an inflammatory reaction occurs in relation to the calcium within the rotator cuff tendon. It is the inflammatory reaction rather than the presence of the calcium that causes the symptoms.
Smaller deposits cause pain if they become acutely inflamed, especially when the calcium salts leak from the lesion into the sensitive bursal tissues.
Pain can also arise with large size deposits which can cause fraying of the rotator cuff tendons as well as inflammation of the subacromial bursa due to mechanical friction against the acromion.
Most early calcium deposits are very soft, much like the consistency of a toothpaste.
After being present for a long period of time, these deposits do dry up and become chalk-like, sometimes even turning to bone.
Patients with calcific tendinitis can have a dull pain which is made worse when the arm is lifted up, especially into overhead positions. It resembles the pain associated with subacromial impingement. The pain is often poorly localised and may be referred down the arm or into the neck.
Patients also have pain at night and may have disturbed sleep. Shoulder movements may be restricted secondary to the progressive thickening and scarring of the bursa.
Some patients can have excruciating pain unrelated to movement. This is believed to be due to the ‘eruption’ of calcific material into the subacromial bursa during the Resorptive Phase. During this phase, the calcium dissolves and as it does, it swells causing extreme and unremitting pain. The pain can be so severe that those affected are often incapacitated by it and describe it as the worst pain they have ever experienced. Often, no shoulder movements are tolerated, and the arm is held firmly against the chest. The pain is usually localised to a specific site of the shoulder and is of shorter duration than the chronic form, with symptoms often settling after 2-3 weeks. But if no intervention is pursued, discomfort can continue for many months.
Calcific tendinitis is diagnosed based on patient’s symptoms, clinical examination and investigations like shoulder x-rays, ultrasound or MRI scans.
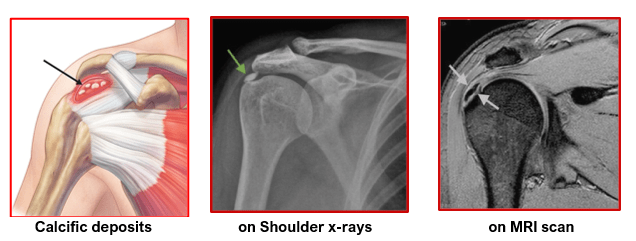
It can often be seen as an incidental finding on x-rays. Shoulder x-rays may need to be taken in different positions to confirm exact location and size of the calcium deposits.
Ultrasound and MRI scans may be needed to see the state of other soft tissues around the shoulder and locate the calcium deposits.
- When a calcium deposit becomes acutely inflamed, either because it ruptures and leaks calcium salts into the bursa or because it pinches the bursa or rotator cuff, the symptoms can be quite severe.
- The acute inflammation can be treated with oral anti-inflammatory medications, localized ice packs and rest in a shoulder sling. If the patient does not have a satisfactory relief with oral analgesics or has excruciating pain, a steroid injection mixed with local anaesthetic is given directly into the subacromial area. This gives faster pain relief. The steroid injection is supplemented by anti-inflammatory medications orally as needed. Steroid injection helps in reducing inflammation and pain over a period of 1 to 2 weeks in acute cases.
- After controlling the acute pain, patients are sent for shoulder physiotherapy. They undergo rehabilitation, as tolerated, to improve their shoulder range of motion, strength and function.
- Non-surgical treatment for calcific tendinitis is highly effective with a success rate of 90 %.
Surgery is needed in patients with calcific tendinitis if:
- There is failure to improve with non-surgical treatments.
- Patient has 2 or 3 recurrent episodes of painful symptoms in the shoulder
- The calcium deposit appears to be enlarging on X-rays and patient has unresolving symptoms.
Calcific tendinitis may need shoulder arthroscopic subacromial decompression and excision (removal) of the calcium deposits.
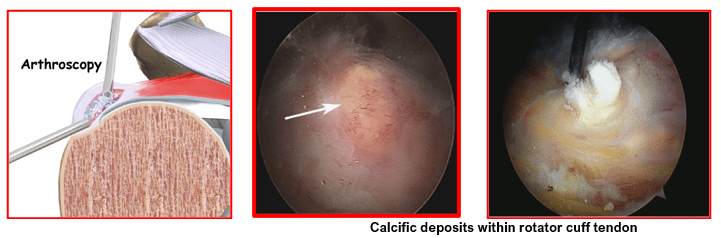
During this keyhole surgery the shoulder joint is thoroughly inspected, and the calcium deposits are located. These deposits are then released from the tendon and removed with specialised instruments. Any inflamed bursa is removed and the space between the tendon and the overlying bone is opened up by removing any tight & thickened ligament along with bony spurs that may be pinching the rotator cuff tendons. This allows the cuff to glide more freely and prevents painful rubbing and inflammation.
Arthroscopic surgery for calcific tendinitis is a safe and reliable operation with over 90 % success rate. It helps relieve patient’s symptoms. They have good pain relief, increased range of shoulder movements and improved strength leading to good shoulder function. It is very rare for calcium deposits to recur in the same shoulder after removal.
- Surgery is done as a day-care or 1 day stay procedure under general anaesthesia with nerve blocks.
- Patients are given a shoulder sling for support for the first few days. They are taught gentle shoulder exercises and allowed to use their hand as tolerated.
- Physiotherapy is to be continued on out-patient basis to improve range of motion, improve muscle strength and regain good shoulder function.
- Pain-killer and anti-inflammatory medications are taken as needed.
- Shoulder ice-packing is done for 4 to 5 times a day.
- Wounds are checked and any sutures removed after 10 days.
- Office work can be started by 1 to 2 weeks.
- Car driving can be started by 2 to 4 weeks when patients are able to handle the vehicle safely
- Heavy lifting, manual work and sporting activities can be resumed after 4 to 6 weeks based on the progress made.
- It can take 3 to 4 months for full recovery after surgery

