
Revision knee surgery or revision total knee replacement is a surgery where a surgeon removes the previous failed implants and replaces them with new implants. This surgery may involve the replacement of one or all of the components.
Revision knee replacement surgery is a complex procedure that requires extensive preoperative planning, specialized implants and tools, prolonged operating times, and an experienced surgeon having mastery of difficult surgical techniques, to achieve a good result.
Revision knee replacement surgery may be advised to patients if they have one or more of the following conditions:
- Loosening of the prosthesis
- Infection in the prosthetic joint
- Worn out prosthesis
- Knee instability or a feeling of giving way while walking
- Dislocation of the prosthesis
- Peri-prosthetics Fractures due to trauma
- Weakening of bone around the knee replacement, a process known as osteolysis (bone loss)
- Chronic progressive joint disease
- Increased pain in the affected knee
- Stiffness in the knee
- Leg length discrepancy
Revision surgery may be needed soon after the original TKR.
The following are reasons for short-term revisions: infection, implant loosening from failed procedure, or a mechanical failure
Reasons for long-term revisions (i.e several years after the original TKR): pain, stiffness, loosening due to wear of mechanical components, dislocation
The surgeon may take risk factors into account in assessing the likelihood of a failed knee prosthesis. Six factors have been identified as increasing a patient’s risk of needing revision surgery within two years of knee replacement surgery:
- Age (Younger patients tend to be more active and to wear out knee prostheses more rapidly than older ones.)
- Prolonged hospitalisation for the original knee surgery
- Concurrent diseases or disorders
- Any type of arthritis
- Surgical complications during the first knee operation
- Having the first knee operation performed at an urban hospital
- Wear and Loosening:Properly functioning implants depend on their appropriate fixation to the bone. Firm fixation is usually achieved by cementing the implant onto the bone. Some surgeons prefer biologic (non-cemented) fixation by using special coated implants that allow bone growth to provide firm fixation and stability. The firmly fixed implants, at initial knee replacement surgery, may become loose over time. Friction caused by the joint surfaces rubbing against each other wears away the surfaces of the implant and forms tiny particles that accumulate around the joint. In a process called aseptic (non-infected) loosening, the bond of the implant to the bone is destroyed by the body’s attempt to digest these wear particles. During this process, the normal bone is also digested which weakens or even fractures the bones. This condition is termed as osteolysis. When the prosthesis becomes loose, the patient may experience pain, change in alignment, or instability. Aseptic loosening is the most common mode of failure of knee implants.
- Infection:Infection is a serious and devastating complication of any surgical procedure. In total knee replacement, the large foreign metal and plastic implants can serve as a surface for the bacteria to latch onto. They form a coating around themselves (biofilm) and become inaccessible to antibiotics. Even if the implants remain well fixed, the pain, swelling, and drainage from the infection make the revision surgery necessary. With current surgical techniques and antibiotic regimens, the risk of infection from total knee replacement is less than 1%.
- Fractures:The location, type and extent of the fracture will determine if revision surgery is needed. Periprosthetic fractures (fractures around the knee implants) can occur due to trauma. This disrupts the implant fixation or changes the stability of the implant which may warrant revision surgery.
- Instability:Instability occurs when the soft-tissue structures, especially the collateral ligaments, around the knee are unable to provide the stability necessary for adequate function during standing or walking. Instability may be the result of increased soft-tissue laxity (looseness), inadequate flexion of the implants, or improper positioning or alignment of the prosthesis. Pain and/or a sense of “giving away” of the knee may alter knee function and require revision surgery.
- Patient-Related Factors:Patient’s Age, activity levels, surgical history and weight can contribute to implant failure. Younger, more active patients have a higher rate of revision than older, less active patients. Obese patients have a higher incidence of wear and loosening. Patients with previous knee surgeries are also at higher risk for infection and implant failure.
After the decision for revision knee replacement is made, standard assessments are performed, including new long leg x-rays, blood tests, and possibly other imaging modalities like bone scans, CT scans, or Magnetic Resonance Imaging (MRI) studies.
X-rays may demonstrate a change in the position or condition of the components. MRI helps to determine the cause, location, and the amount of bone loss before surgery.
Aspiration of the knee (joint fluid removed with a needle) may be required if infection is suspected. This aspirated fluid will then be sent to a laboratory for analysis to identify the specific type of organism causing infection.
- Steps involved in a revision total knee replacement:
- Most Revision Total Knee Replacements take longer to perform than primary procedures (about two to three hours).
- It may involve the replacement of one or all of the components.
- The surgery is performed under long acting spinal, epidural or general anaesthesia.
- The surgeon makes an incision over the knee, preferably through the old scar, to expose the knee joint.
- The Patella (kneecap) along with its ligament are be moved aside to create space for performing the revision surgery.
- The first step is removal of the implant. The old femoral component of the knee prosthesis is removed first using special cutting devices.
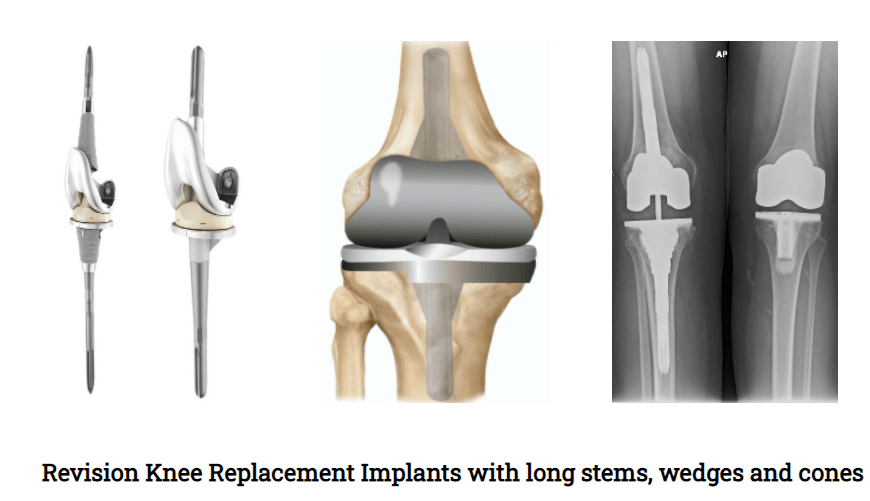
- The femur then is prepared to receive its new prosthesis. In some cases, the damaged bone gets removed and bone grafts or metal wedges may be used to reconstruct the lost bone and strengthen the femur. In extensive bone loss cases, specially coated metallic cones are used for reconstruction of the femur. Additionally, long supporting rods (intra-medullary stems) are attached to the implant to provide extra fixation to the implant and stability to the joint.
- Next the tibial component along with the old plastic liner is removed.
- The damaged tibial bone is cut and prepared to receive its new prosthesis. Similar to the femur, metal wedges, bone grafts, long stems or special cones may be used to reconstruct and strengthen the tibia, depending upon the loss of bone.
- If the patella (kneecap) has been damaged, the surgeon will prepare the patellar bone for attachment of a new a plastic component with bone cement.
- Appropriate size femoral, patellar and tibial implants, without cement, are attached to the bones. Then a plastic liner of sufficient height is used to provide a stable joint. After all trials are in place, good range of motion and patellar tracking are confirmed.
- After this confirmation all trial implants are removed. The femoral, tibial and patellar bones are thoroughly washed out and dried in preparation for bone cementing the new implants. Femoral, tibial and patellar implants are secured to the bones using bone cement.
- The new plastic liner of correct size is firmly secured on top of the tibial component. The tibial, femoral and patellar implants are then brought together to form the new knee joint. Joint stability, range of movements and patellar tracking are re-confirmed.
In cases with extensive bone loss or absence of the supporting collateral ligaments, hinged types of implants are used. Hence operating surgeon needs to have all types of implants and inventory ready in the operation theatre which enables him to use the most appropriate revision implants for the patients. This ensures best possible outcome for the patient.
- At the end the joint is thoroughly washed out, any bleeding points are secured and sealed with cautery to avoid bleeding.
- The wound is then closed in layers after keeping a suction drain inside to drain out excess blood from the knee.
- Sterile dressings and a compression bandage are applied. Patients are also provided with a long leg splint for initial support.
Post-operative care after knee revision surgery is very similar to the care of a primary knee replacement. This includes a combination of pain medication and blood management as necessary. Physiotherapy is started after few hours post-surgery to encourage ankle and toe movements. Appropriate antibiotics and some method of blood clot prevention (DVT Prophylaxis) will be continued in the postoperative period. A brace or splint may be used to protect the joint after the surgery.
In most cases, physiotherapy will be initiated within 24 hours of the procedure. In some cases, protective weight bearing with a knee brace, such as Partial Weight Bearing (PWB) or Toe Touch Weight Bearing (TTWB), is needed to promote bone healing. Therapy will usually continue for up to three months following the surgery. Assistive devices, such as a walker or crutches, will be used early in the post-surgery phase, and patients will progress to a stick or unaided walking as their condition and confidence improves.
Patient’s hospital stay can be between 3 to 5 days depending upon the complexity of the case.
Recovery time after revision knee surgery is variable depending upon several factors. Patients should be forewarned about this recovery duration.
Any surgery can have potential complications. The complexity of revision joint surgery increases the chance of surgical complications which are similar to the primary TKR.
Possible complications include:
- Infection
- Bleeding
- Damage to nerves or blood vessels
- Intra-operative fractures – occur during removal of the old implants or the insertion of new ones
- DVT (Deep Venous Thrombosis) or blood clots
- PE (Pulmonary Embolism)
- Implant loosening, especially in overweight patients
- Dislocation of the new implants. (Higher compared to primary TKR).
- Additional or more rapid loss of bone tissue
- Difference in leg length resulting from shortening of the leg with the new prosthesis
- Formation of heterotopic bone, which is bone that develops at the lower end of the femur following surgery. (Joint infections after surgery increase risk for this)
Infection, bleeding, damage to nerves or blood vessels, and intra-operative fractures can be minimized by use of antibiotics before and after surgery, sterile surgical techniques and utilizing well-planned surgical exposures.
Similar to primary TKR, some mild swelling of the knee or ankle may be present after surgery for as long as 3 to 6 months. Swelling can be treated by elevating the leg, applying an ice pack, and wearing compression stockings.
Pre-existing medical conditions, such as heart and lung complications, or stroke conditions, can be aggravated by a revision procedure. These conditions may also develop in patients after revision surgery. Very rarely, death can occur. The decision to perform revision joint surgery is made when the benefits of pain relief and functional improvement outweigh the risk of potential complications.
Total knee replacement (TKR) surgery is a very is a common surgery performed for advanced knee arthritis. It gives significant improvements in knee pain, mobility, function and quality of life. Outcomes following TKR are generally excellent in the majority of the patients.
Infection after TKR is rare and occurs in less than 1 % of patients undergoing primary TKR. But it remains a challenging problem that can be difficult to diagnose and treat.
A TKR may become infected due to the presence of bacteria around the knee soft tissues, the artificial implants and the underlying bones. This can lead to bone destruction, implant loosening, deformity of the affected leg and poor quality of life due to pain and reduced mobility.
Infection can set in during the time of surgery, or anywhere from weeks to years after the surgery.
The most common ways for harmful bacteria to enter the body and cause the infection are:
- Through the surgical incision made for the TKR or through any breaks or cuts in the skin
- During major dental procedures (such as a tooth extraction or root canal). Bacteria get carried to the knee via the bloodstream.
- Through wounds from other surgical procedures
After reaching a person’s new artificial knee joint, the bacteria may multiply and cause an infection.
Some bacteria are harmless, such as those that occur naturally in the stomach, while others may harm a person and cause an infection. A person’s immune system usually kills any harmful bacteria that get into the bloodstream. When a person has a knee replacement, their knee joint is replaced with an artificial joint made of metal and plastic. These materials are not organic and hence it is harder for the body to kill the bacteria stuck on them.
Anyone who has a knee replacement can develop an infection after surgery, but some groups are at a greater risk of infection. These include people who:
- have immune deficiencies, such as HIV or lymphoma
- have diabetes
- have poor circulation in their hands or feet
- are using treatments that suppress the immune system, such as chemotherapy or corticosteroids
- have frequent urinary tract infections
- have a BMI of over 50
- have dental problems
- have dermatitis or psoriasis
- have rheumatoid arthritis
- smoke or chew tobacco
- have undergone knee surgery previously
- have had an infected TKR previously
The TKR infection may be superficial during the early phase of 2 to 4 weeks post-surgery and be limited to the subcutaneous tissues only without any breach of the deep fascia.
If the infection breaches the deep fascia and goes deeper, it becomes a deep infection. This can generally happen 4 to 6 weeks after surgery. It involves the deeper tissues and also spreads around the implants used for replacing the knee joint. It can go onto involve the underlying bones as well.
The symptoms and signs of infection after TKR are:
- Increased pain or stiffness in a previously well-functioning knee joint
- Difficulty in walking and weight bearing
- Swelling
- Warmth and redness around the wound
- Wound drainage
- Fevers, chills and night sweats
- Fatigue
- Patient may be walking with a limp
- Deformity of the knee
- Presence of any wounds (sinuses) with or without discharge
- Knee may be tender and have painfully limited knee movements
- It may be unstable on stressing the joint
Infection after TKR is based on patient’s complaints, his physical examination, X-rays, blood tests, MRI or CT scan, Bone scan and knee joint fluid aspiration.
Specific blood tests can help identify an infection. 3 blood tests are routinely performed for patients with suspected infection of TKR. Haemogram (complete blood cell count – CBC), Erythrocyte Sedimentation Rate (ESR) and C-reactive Protein (CRP). Haemogram helps to monitor the white cell count. The ESR and CRP tests measure the level of inflammation in the patient’s body. Although neither test will confirm the presence of infection, if either or both of them are elevated, it raises the suspicion that an infection may be present. If the results of these tests are normal, it is unlikely that the patient’s joint is infected.
Aspirated fluid from the knee joint can help identify an infection. Under strict sterile conditions and with proper aseptic precautions, a needle to inserted to draw fluid from the knee joint. The fluid is sent to the laboratory for examination under microscope for presence of any micro-organisms. The samples are also cultivated and monitored to see if any bacteria or fungus grow from the fluid.
The joint fluid is also analyzed for the presence of white blood cells. In normal knee fluid, there are a low number of white blood cells. The presence of a large number of white blood cells (particularly cells called neutrophils) indicates that the joint may be infected. The fluid may also be tested for specific proteins that are known to be present in the setting of an infection.
The treatment options available for managing an infected TKR patient are:
Non-surgical (conservative) and Surgical Treatments.
Non-surgical (conservative) Treatment: useful in a limited group of patients who have superficial infection. The skin or the subcutaneous layers are involved without involvement of the deep fascia or underlying deeper tissues or the artificial joint implants. Such cases need to be diagnosed quickly and their treatment started as soon as possible. This involves administration of intra-venous or oral antibiotics for 5 to 7 days. Early treatment in such patients with superficial infection helps in controlling the infection and allows healing with good success rate.
Surgical treatment: is invariably needed for patients presenting late and in those patients in whom the infection has now involved the deeper tissues and also the knee implants.
There are two types of surgeries commonly performed for managing an infected TKR.
Debridement:
This procedure involves surgical washout of the joint. It is done for deep infections in a TKR that are picked early (within several days of their onset), and those that occur within weeks of the original surgery. This can be within first 2 to 4 weeks post-surgery. Deep infections that are caught very early, may sometimes be cured with joint debridement.
During this procedure, called debridement, the surgeon reopens the surgical wound to gain access to the knee joint, then he removes all contaminated soft tissues. Fluid and tissue samples are collected to confirm presence and type of micro-organisms causing the infection. The metallic implants are thoroughly cleaned with sterile normal saline, and the plastic liner or spacer between the femoral and tibial implant is exchanged for a new one. The wound is then closed in the usual manner over a deep wound drain that gets removed after 24 to 48 hours. Patients are given suitable intravenous (IV) antibiotics for approximately 6 weeks. These need to be changed or continued as per antibiotic sensitivity reports from the labs.
Staged surgery: Involves 2 Stage surgical plan
Infections that have been present for longer periods of time (more than 6 weeks) and Late infections (those that occur months to years after the joint replacement surgery), almost always, requires a two staged surgical plan.
In general, the longer the infection has been present, the harder it is to cure without removing the implant. The bacteria adhere to the implants and form an impregnable biofilm layer around themselves. The biofilm does not allow any antibiotics to reach the bacteria. The biofilm is also difficult to be scrubbed off the implants and the underlying bones. Hence complete implant removal remains the best option to control infection.
The FIRST STAGE of this staged revision surgery includes:
- Removal of the artificial joint: This is done with help of specialised instruments whilst taking care to avoid damage to the underlying bones and maintain the bone stock.
- Soft tissue debridement and Joint washout: helps get rid of infected soft tissue in the joint.
- Placement of antibiotic spacer: This helps to maintain the joint space, prevent soft tissue scarring and keep the joint aligned while the infection is being treated. Articulating specialised spacers also allow knee movements and weight bearing. Spacers are made with bone cement that is loaded with antibiotics. These antibiotics flow into the joint and surrounding tissues and, over time, help to eliminate the infection.
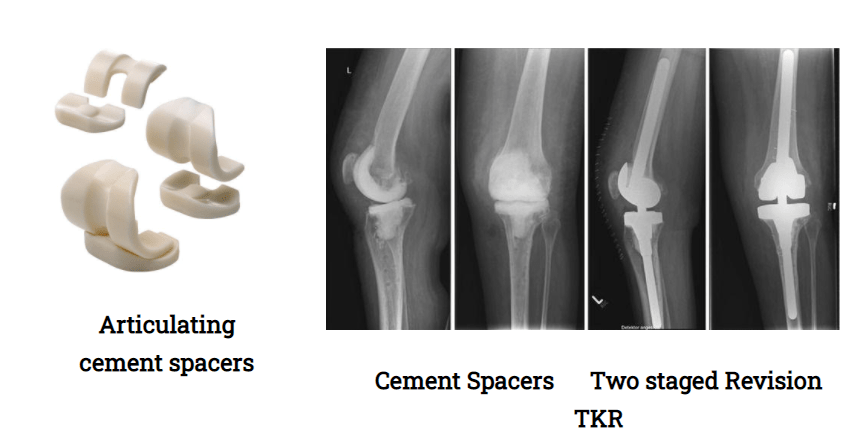
- Antibiotic Therapy: Patients who undergo staged surgery typically need at least 6 weeks of IV antibiotics, or possibly more, before a new joint replacement can be implanted. Orthopaedic surgeons have to work closely with their microbiology colleagues, for their help and guidance, for choosing the right and most effective antibiotic, the best method of its administration (oral or intravenous) and the duration of the antibiotic therapy. Serial blood tests are done for monitoring the response to these antibiotics and also to note if any untoward side-effects are occurring in the body. Normally 6 weeks of antibiotics are given intra-venously.
SECOND STAGE:
This second stage of revision surgery involves the insertion of new knee replacement implants
This stage is generally performed 6 weeks after the first stage. The blood counts have to be satisfactory and normal. This indicates that the joint infection has come under control. Patient should also be optimally fit to undergo this second stage.
The knee joint is exposed, the spacers are removed, the joint is debrided and washed out. The bones are prepared to receive the new implants. Depending upon the status and deformities of the femur and tibia, additional stems, wedges or cones are used, as needed, to provide a stable knee with good range of knee motion and normal patellar tracking. Hinged implants are used for patients with inadequate bone stock along with incompetence or loss of the collateral ligaments. New implants need to be cemented in place with their extension stems (rods) to give improved and stronger fixation and stability. Wounds are closed in the standard manner over a deep drain in the knee. A knee brace is also provided depending upon complexity of the procedure.
SINGLE STAGED SURGERY: During this single staged surgery, the implants are removed, the joint is thoroughly debrided (including the soft tissues and bones), the bones are reshaped and prepared to take the new implants. The new implants are inserted as usual, all in a single stage. The wounds are closed over a drain as usual.
Single-stage surgery is still not as popular as the two-stage surgery. But it is gaining wider acceptance as a method for treating infected total joints. It is more popular in Europe (especially, Germany). Surgeons are still observing the studies and outcomes of single stage revision joint replacements.
The following steps and precautions may help in reducing the risk of infection in a patient undergoing knee replacement surgery:
- Using prophylactic antibiotics: Preventive medicines may help reduce the risk of knee replacement infection. We usually give three doses of intra-venous antibiotics within first 24 hours with the first dose given 20 to 30 minutes before skin incision is taken.
- After their TKR, patients may also need prophylactic antibiotics for other surgeries like dental work.
- Keeping operation time short: Surgeon should be experienced and sleek in his surgery to keep the operating time short. This helps to reduces the length of time the wound is open and vulnerable to infection.
- Reducing the number of people present: Limiting the number of people and limiting the number of times they come and go may reduce the bacterial counts in the room and decrease the risk of infection.
- Using sterile equipment: The operation theatre and surgical instruments should all be thoroughly sterilized. The instruments should not be exposed to any contamination. The implants used during surgery should be in pre-sterilised airtight packages. Before using them, their sterility should be confirmed and maintained throughout the surgery. All staff involved in the joint replacement surgery must use disposable drapes and surgeon gowns. They must change gloves frequently as needed during the surgery.
- Screening for bacteria in the nose: If a person has certain types of harmful bacteria in their nasal passage, they may increase the risk of infection. Some hospitals screen for these bacteria before operating. If harmful bacteria are found, the person will be given an antibacterial ointment to use. Some hospitals will routinely decolonize nasal passages with mupirocin several days before surgery.
- Washing with chlorhexidine: This may help reduce the number of harmful bacteria on the skin before surgery.
- Thorough skin cleaning in OT: The operative leg including foot must be thoroughly cleaned before surgical preparations. This also helps to control risk of infection.
- Having standardised protocols: Wards and OTs for joint replacement surgeries should follow standard protocols which help in maintaining discipline from all concerned staff and bring in uniformity in precautions to be taken during knee replacement surgeries.
- After a TKR, following measures may help reduce the risk of infection:
– Following the surgeon’s advice on how to treat the wound
– Clean and cover cuts, wounds, or burns as soon as they happen
– Maintain dental hygiene, as infections in the mouth may spread to the
artificial joint
More than 90% of patients who undergo revision procedures can expect to have good to excellent results. Although expected outcomes include pain relief with increased stability and function, complete pain relief and restoration of function is not always possible. 5% to 20% of patients may still experience some pain following revision knee surgery. This can persist for several years after the procedure.
Knee arthrodesis and Above knee amputation are the two surgical alternatives to revision knee surgery. They are rarely used, since they can sometimes be more complex and lead to worse results than revision surgery.
With arthrodesis or knee fusion the pain may be relieved, but at the expense of keeping the knee in a straight position. The knee is not able to bend after fusion. Knee arthrodesis can be done using either a very long intra-medullary nail or an external fixation type device.
Above knee amputations may be used in cases of severe joint infections that cannot be eradicated.
After weighing the alternatives, considering the higher rate of complications as compared to primary knee replacement, most patients and surgeons prefer revision surgery to these above surgical options.

