
Knee osteotomy is a surgery that involves cutting of a bone to correct the alignment of the knee and improve its function. It is recommended for patients having pain and instability due to damage or arthritis affecting only one side (compartment) of the knee joint.
In a varus knee, there is bow leg deformity with arthritis affecting the inner or medial compartment of the knee joint. As a result, more stress goes through the inner side causing wear and tear of the knee joint cartilage.
In a valgus knee, there is knock knee deformity affecting the outer or lateral compartment of the knee joint. Here there is more stress on the outer compartment leading to early wear and tear
During knee osteotomy, the surgeon strategically cuts the bone and alters the mechanically alignment or shape of the legbone. The patient’s body weight is now shifted from the affected side towards the healthy side. This leg realignment helps to off-load the stress on the arthritic side leading to pain reduction, improved mobility and function. Knee osteotomy helps to slow down the damage to the joint cartilage and delays the need for knee joint replacement surgery for many years. Knee osteotomy can allow a person to lead a very active lifestyle including high impact exercises
The two main types of osteotomy are: the opening wedge and the closing wedge. These osteotomies are commonly performed at the upper tibia or at the lower femur.
In a closing wedge osteotomy, the surgeon removes a wedge shape piece from the cut bone. The cut surfaces of the bone are then brought together thus closing the osteotomy space.
In the open wedge osteotomy, the surgeon cuts the affected bone and creates a wedge shape gap between the cut surfaces. This gap is either left open or filled with appropriate size bone graft to hold the osteotomy open and also assist in healing of the bone cut.
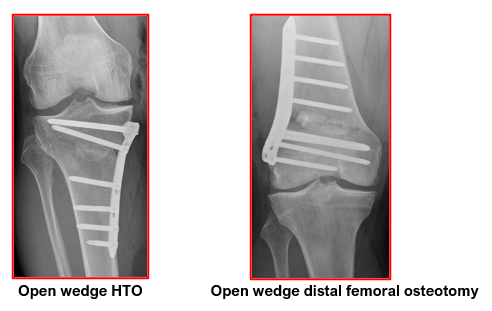
The high tibial osteotomy (HTO) of the upper tibia is a routinely performed surgery that helps to relieve pain, improve function and correct bow-legged alignment. This can be an open wedge or a closing wedge osteotomy.
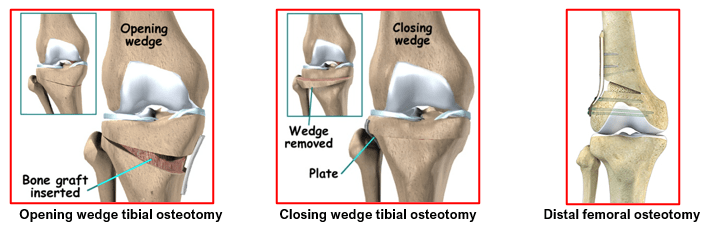
In a similar way, the lower femoral osteotomy is performed, though less commonly, to help relieve pain, improve function and correct knock-kneed alignment.
Knee osteotomy is ideally recommended for patients who:
- Have mild to moderate arthritis affecting only one side of the knee and little to no damage on the other side.
- Are relatively young (40 to 60 years of age)
- Are not overweight
- Have good knee mobility. They should be able to straighten their knee fully and bend it at least to 90 degrees
- Have significant arthritis pain that is brought on by activity or standing for long periods of time.
- Want to stay physically active and are willing to commit to a long post-surgical physiotherapy regimen
- Are able to use crutches and limit weight bearing for 6 to 8 weeks after the surgery
The surgeon takes a detailed medical history from the affected patient including recent treatments for knee problems. Both the knees are thoroughly examined. The spine, hips and ankle joints are also checked. Long leg x-ray of the lower leg during standing are advised. These help in judging the severity of the knee deformity and also helps in the preoperative planning. The size of bone wedge to be removed or created gets calculated.
Appropriate blood tests for anaesthesia fitness are done. Additional investigations like ECG, Chest x-ray and 2D Echocardiography may also be done based on patient’s age and presence of any medical problems.
Preoperative CT scans and MRI of the knee may be needed in some patients with complex deformities or history of injury. The status of knee cartilage and surrounding ligaments is seen on the MRI scans.
Patients are properly counselled and consented for their surgery. The surgery is performed under spinal or general anaesthesia. Thigh tourniquet is used for this surgery. The whole procedure may take 1 to 2 hours.
The osteotomy sites are pre-marked on the leg after thorough sterile painting and draping. Some surgeons perform a quick arthroscopic assessment of the knee initially. This helps to see the status of the good compartment of the knee. Any minor issues with knee cartilage or meniscus are dealt with at the same time to give better results after surgery. Surgery proceeds only if the good compartment has a healthy cartilage.
Skin incisions are taken as planned. The bone is exposed. Guide wires are inserted into the tibia /femur under x-ray control. The size of the wedge to be added or removed depends on the patient’s anatomy and degree of bow-legged or knock-kneed deformity. Typically, a 1 mm wedge will provide 1 degree of correction, so a 10 mm wedge will provide a 10-degree change in knee alignment.
Appropriate osteotomy is then performed under x-ray control. Once the osteotomy is done, either a closing wedge or an open wedge, the cut bones are held together and stabilised with specialised plates and screws. Final confirmation of the corrected alignment is seen on the image intensifier.
Wound are closed with dissolving sutures and tapes. Sterile dressings are put on and a compression bandage is given. Patients get transferred to the recovery ward for observation.
- Patients can start eating and drinking after 3 to 4 hours. They are given icepacks and leg elevation to reduce knee swelling. Appropriate painkillers are given.
- Antibiotics are given for first 24 hours only.
- Patients are encouraged to start moving their ankle and do static quadriceps exercises.
- They get mobilised with help of elbow crutches or a walker. They are partial weight bearing for the first 6 weeks. Knee range of motion exercises are allowed freely as tolerated. Patients are given a hinged knee brace for protection.
- They should be able to – get in and out of bed independently, use the commode, walk safely with crutches, use staircase before getting discharged from the hospital, in 2-3 days.
- Their operative wound gets checked at 2 weeks and physiotherapy is carried on an OPD basis.
- Patients get knee x-rays done at 6 weeks and 3 months. The osteotomy starts healing by 6 weeks and consolidates by 3 months.
- They may take 4 to 6 months to feel the full benefit of their knee osteotomy surgery.
In the ideal patient with the correct indications, an osteotomy is a good operation for reducing pain and improving knee function. It may delay the need for knee replacement surgery. The success of an osteotomy still providing good function and pain relief at five years is approximately 85%, 70% at ten years, and about 50% at 15 years.
Most people after an osteotomy can return to sport somewhere between six to nine months. This will depend on your pre-operative level of activity, the severity of arthritis of your knee, as well as the progress you make with your rehabilitation.
For an office type job, you may be able to return to work between two and three weeks. But if your occupation requires a lot of walking or heavy manual labour, then your return to work may be delayed for 6 to 12 weeks.
An osteotomy has a good chance of delaying the need for a knee replacement in the future. Most people down the track will develop arthritis in other parts of the knee or have arthritis that progresses within the same compartment of the knee. When this occurs, you may require a total knee replacement.
Most people who have an osteotomy require removal of the plates, commonly between one and two years after their operation. This is performed as a day operation and the recovery time is minimal. It is safest to have the plates removed at this time so that when surgery is performed in the future, there are no plates that could interfere with further treatment.
Most people will have some pain for 3-4 weeks after an osteotomy. This is generally well controlled with oral medication. Once the osteotomy heals fully, the majority of the arthritis pain symptoms will improve significantly as weight is carried on the healthier cartilage of the unaffected compartment.
The possible risks or complications after any knee osteotomy are: swelling, stiffness, ongoing pain, damage to blood vessels or nerves, deep vein thrombosis, infection, failure of the osteotomy to heal, failure of the osteotomy fixation implants, fractures around the osteotomy, progression of arthritis despite the osteotomy and need for knee replacement in future.

