
The biceps tendon is a long cord-like structure located in the front of the shoulder. It arises from the top of the glenoid (shoulder socket) and exits the joint through a bony trough called the biceps groove. Below the shoulder, this tendon becomes the long head of the biceps muscle. The short head of the bicep is a continuation of the conjoined tendon, which originates from the coracoid (a bony hook at the front of the shoulder blade). The biceps muscle has two anchor points in the shoulder region, and it helps to flex (bend) the elbow and rotate the forearm.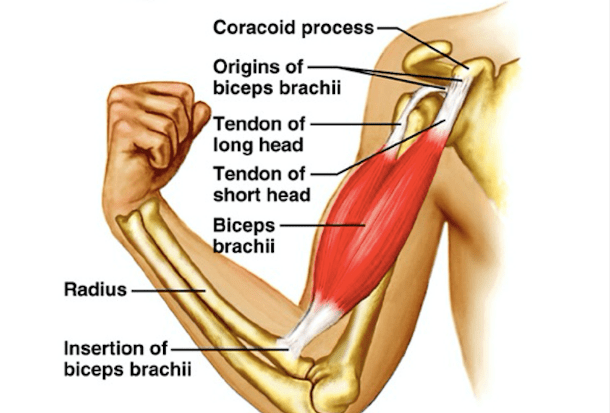
Biceps tendon injuries occur commonly with increasing age. With ageing there is loss of tendon elasticity and they become stiffer and brittle. In addition, there is reduction in the blood supply to the tendon with increasing age. This degenerative process is more pronounced in sedentary individuals. It can be lessened with proper and regular exercises. But even well-trained individuals and athletes, can get biceps tendon injuries. An otherwise healthy tendon can get damaged due to overuse and overtraining.
Ageing, inactivity, or over-activity can weaken the biceps tendon. It becomes prone to injuries due to reduced ability to tolerate repetitive actions and also sudden loads.
Some patients develop bone spurs in their bicipital grooves or under the top of their shoulder blades (the acromion). This causes friction of the tendon against these bony spurs leading to wear and tear of the tendon.
In some patients there is a dislocation of the biceps tendon from its groove. This is usually seen in combination with a tear of the subscapularis tendon or the rotator cuff tendon, which normally help in keeping the biceps tendon in it groove.
The biceps tendon can also be injured at its attachment site on top of the glenoid. This usually involves an avulsion, where the tendon is pulled off the bone and rendered unstable.
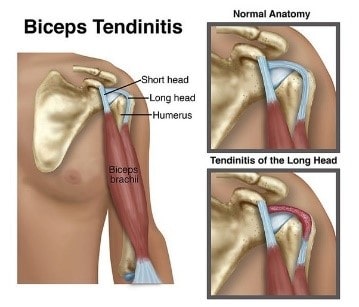
Irritation of the biceps tendon or its sheath causes tendon inflammation. This causes pain and swelling. This condition is known as tendinitis.
Mild injuries can also result in microscopic tearing of individual tendon fibres. With severe injuries, larger tears can occur. The biceps tendon can be partially torn or even completely ruptured. If a complete rupture occurs, the long head of biceps tendon will usually fall distally toward the elbow. Bicep muscle function usually remains nearly normal because of its dual attachment proximally.
Biceps tendon problems are diagnosed based on patient’s medical history, thorough clinical examination and appropriate investigations.
Patients complain of pain located to the front of the shoulder and associated with overhead activities and also lifting.
There is tenderness on probing the front of the shoulder and also pain on certain provocative shoulder manoeuvres. There can be associated shoulder weakness if rotator cuff tendons are also inflamed or torn. In patients with complete rupture of their biceps tendon, there is a visible and palpable lump in the arm especially on bending the elbow (pop-eye sign).
Shoulder x-rays show presence of any bony spurs at the acromion (shoulder tip) or the bicipital groove.
- Rest, Ice packs and anti-inflammatory medications are needed, initially.
- If pain persists then a steroid injection is needed to control the pain and swelling.
- Severe cases, that fail to improve despite above conservative measures, may require arthroscopic surgery.
Surgical treatment depends on the nature and extent of damage to the tendon.
If only a small portion of the tendon is damaged, a simple arthroscopic shaving (debridement) of the torn fibres is needed. This helps reduce pain and improves function.
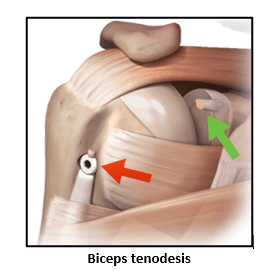
If a significant portion of the tendon is involved, a biceps tenodesis procedure needs to be performed. In this surgery the biceps tendon is removed from its original attachment to the top of the glenoid and is re-attached to the upper humerus using special devices like suture anchors or screws. This allows the biceps tendon to heal at a new location, the biceps muscle also maintains its functional length and function. There is reduction of patient’s pain and his shoulder function returns back to normal. Young patients are ideal candidates for this surgery.
If the biceps tendon is completely ruptured and causes the muscle to bulge in the upper arm (pop-eye sign), a biceps tenodesis procedure is performed, especially in younger patients. This, however, needs presence of the torn upper end of the tendon to be easily traceable for re-attachment.
A biceps tenodesis is cannot be done if the tendon slides too far distally and remains immobile or if patients present late after their injuries. In delayed cases the tendon is scarred, immobile and stuck to its surrounding tissues making its re-attachment impossible.
In elderly patients, with significant tendinitis and fraying of the biceps tendon, a biceps tenotomy procedure can be done. Here the biceps tendon is cut from its attachment site from the glenoid socket and the tendon end is allowed to slide down. There is reduction of shoulder pain and improved function in this group of patients. But they have to bear with the cosmetic deformity of upper arm bulge (pop-eye sign) and need to be counselled about this prior to their surgery.
If the tendon has been partially avulsed from its origin on the top of the glenoid along with the labrum (SLAP lesion), then it is arthroscopically re-attached using tiny suture anchors (SLAP Repair).
- Patients can be discharged home same day or the next day.
- A simple shoulder sling is provided for 3 to 4 weeks.
- Pain-killer and anti-inflammatory medications are taken as needed.
- Ice packs are used for 4 to 5 times day.
- They can start desk type work after 1 -2 weeks
- Gentle shoulder pendulum exercises are done 2 to 3 times a day. Physiotherapy is needed for 2 to 3 months.
- Tendon healing takes 6 to 8 weeks. Overhead activities are permitted after 6 weeks.
- But heavy lifting is to be avoided for 3 months.
- Unrestricted activities, needed for work or sports, are permitted after 3 to 4 months of shoulder rehabilitation.

